

-(43).png)
-(42).png)
-(40).png)
-(44).png)
You Don't Need to Calm Down
Stress is something we all feel. And while it’s a universal feeling...
-(31).png)
"I have been a patient safety activist for 14 years since the death of my 19-year old son due to profoundly uninformed and unethical care in his college town. In 2013, I wrote a seminal article published in the Journal of Patient Safety, in which I estimated that 440,000 Americans die prematurely each year because of preventable events initiated in hospitals."[1] —John T. James, Ph.D.
"We have not as a country recognized the endemic problem of people dying from the care that they receive rather than the illness or injury for which they seek care."[2] —Martin Makary, MD, MPH, Johns Hopkins University School of Medicine
"It’s public pressure that brings about change. Hospitals have no incentive to publicize errors; neither do doctors or any other provider." [3] —Jim Rickert, MD
For nearly half a century, a growing body of research has quietly accumulated a disturbing picture of modern medicine. While the healthcare system is rightly celebrated for its life-saving interventions (emergency surgery, advanced diagnostics, etc.), a parallel literature has documented a darker reality: medical care itself is a leading cause of death in the United States.
The evidence is not new. It stretches from a 1974 Journal of the American Medical Association article warning of tens of thousands of annual drug-induced deaths to a 2016 British Medical Journal study concluding that medical error is the third leading cause of death in America. Between these bookends, the Institute of Medicine, the Department of Health and Human Services, and numerous independent researchers have consistently found that preventable harm in healthcare settings kills anywhere from 44,000 to over 400,000 Americans each year.
These numbers are not merely academic. They represent real patients—people who entered hospitals, nursing homes, and doctors’ offices seeking healing, only to be harmed or killed by the very system designed to help them. The causes are diverse: adverse drug reactions, surgical errors, hospital-acquired infections, medication mistakes, unnecessary procedures, and the cascading complications of iatrogenic illness.
Yet despite decades of documentation, official mortality statistics from the Centers for Disease Control and Prevention (CDC) do not list “medical error” or “adverse drug reaction” as causes of death. The coding system used for death certificates was designed for billing, not for capturing iatrogenic harm or the complex causal chains that lead to death. As a result, these deaths are attributed to the underlying diseases being treated, effectively disappearing underlying health-related issues from public health awareness and policy prioritization. The patient who dies from malnutrition in a nursing home is counted as a dementia death. The patient, whose undiagnosed vitamin D deficiency contributed to a fatal fall, is counted as an accident. The patient whose medication-induced arrhythmia causes cardiac arrest is counted as a heart disease death.
What follows is a chronological summary of key findings from major studies published between 1974 and 2022. Together, they paint an unmistakable picture: the American medical system, for all its advances, remains a significant and underappreciated cause of preventable death—and the way we track mortality actively conceals this reality.
Summary of Key Study Findings
1. 1974 – Talley & Laventurier, Journal of the American Medical Association[4]
Finding: An estimated 60,000 to 140,000 deaths annually from adverse drug reactions (ADRs).
Significance: This was one of the earliest major warnings about drug-induced mortality. The authors explicitly noted that their estimate was “probably extremely conservative” because they had no data measuring drug-induced deaths in ambulatory (outpatient) and extended care populations. In other words, the true toll was likely much higher even then.
2. 1996 – Johnson & Bootman, Journal of Managed Care Pharmacy[5]
Finding: Deaths owing to drug-related problems (DRPs) ranged from 79,000 to 198,815 deaths annually.
Significance: This analysis confirmed that the problem identified in 1974 had not abated. The wide range reflects different methodological approaches, but even the lowest estimate exceeded many recognized causes of death. The study helped establish drug-related mortality as a persistent, large-scale public health crisis.
3. 1999 – Institute of Medicine, “To Err Is Human.”[6]
Finding: At least 44,000 to 98,000 Americans die each year as a result of medical errors. Using the lower estimate, deaths due to medical errors exceed those from motor vehicle accidents (43,458), breast cancer (42,297), and AIDS (16,516).
Significance: This landmark report brought patient safety into the national spotlight. For the first time, a prestigious federal advisory body declared that medical errors were not rare anomalies but a leading cause of death. The report’s title—”To Err Is Human”—framed the problem not as individual incompetence but as a systemic failure requiring systemic solutions. It catalyzed patient safety research and policy, though subsequent studies would show that progress remained frustratingly slow.
4. 2000 – Starfield, Journal of the American Medical Association[7]
Finding: A comprehensive tally of iatrogenic (medically caused) deaths totaled 225,000 per year from:
Significance: Starfield’s analysis was a landmark synthesis, combining multiple categories of harm into a single estimate. It directly challenged the notion that the US healthcare system was “the best in the world” (the title’s question). By showing that iatrogenic deaths alone rivaled heart disease and cancer as leading killers, Starfield forced a reckoning with the gap between medicine’s self-image and its actual performance.
5. 2010 – Department of Health and Human Services, “Adverse Events in Hospitals.”[8]
Finding: Among Medicare beneficiaries, 1.5 percent experienced an event that contributed to their deaths. This projects to 15,000 patients in a single month—or approximately 180,000 deaths per year.
Significance: This was not an independent study but a federal government report. The fact that 180,000 Medicare patients (extrapolated annually) experienced fatal adverse events while in hospital care represented an official admission of a systemic problem.
6. 2013 – Light et al., The Journal of Law, Medicine & Ethics[9]
Finding:
Significance: This study shifted focus from medical errors in general to pharmaceutical harm specifically. The finding that 20% of new drugs eventually prove dangerous enough to require black-box warnings or withdrawal is a stunning indictment of the drug approval and surveillance system. The authors explicitly framed this as “institutional corruption,” arguing that the pharmaceutical industry’s influence over regulation, research, and clinical practice systematically prioritizes market access over patient safety.
7. 2013 – James, Journal of Patient Safety[10]
Finding: An evidence-based estimate of over 400,000 deaths per year from patient harms associated with hospital care.
Significance: James’s analysis produced the highest credible estimate to date. His most important contribution, however, was methodological and philosophical: “Whether the true number is 100,000, 200,000, or 400,000 Americans each year is, in a sense, beside the point—any of these figures demands assertive action.” The study was a frustrated response to the slow pace of change following the 1999 IOM report. By pushing the estimate to 400,000, James sought to finally “foster an outcry for overdue changes.”
8. 2016 – Makary & Daniel, British Medical Journal[11]
Finding: A mean rate of 251,454 deaths per year from medical error, based on studies published since the 1999 IOM report, extrapolated to 2013 hospital admissions.
Significance: This is among the most recent and widely cited major estimates. The authors explicitly compared their figure to CDC rankings and concluded that medical error is the third leading cause of death in the United States, behind only heart disease and cancer. They noted that their figure likely understates the true incidence because it relies on errors extractable from documented health records and includes only inpatient deaths—excluding outpatient clinics, nursing homes, and ambulatory surgery centers. The study’s publication in the BMJ (a leading general medical journal) gave the finding mainstream credibility. The authors’ core argument—that the absence of national data on medical error is itself a public health scandal—remains unanswered.
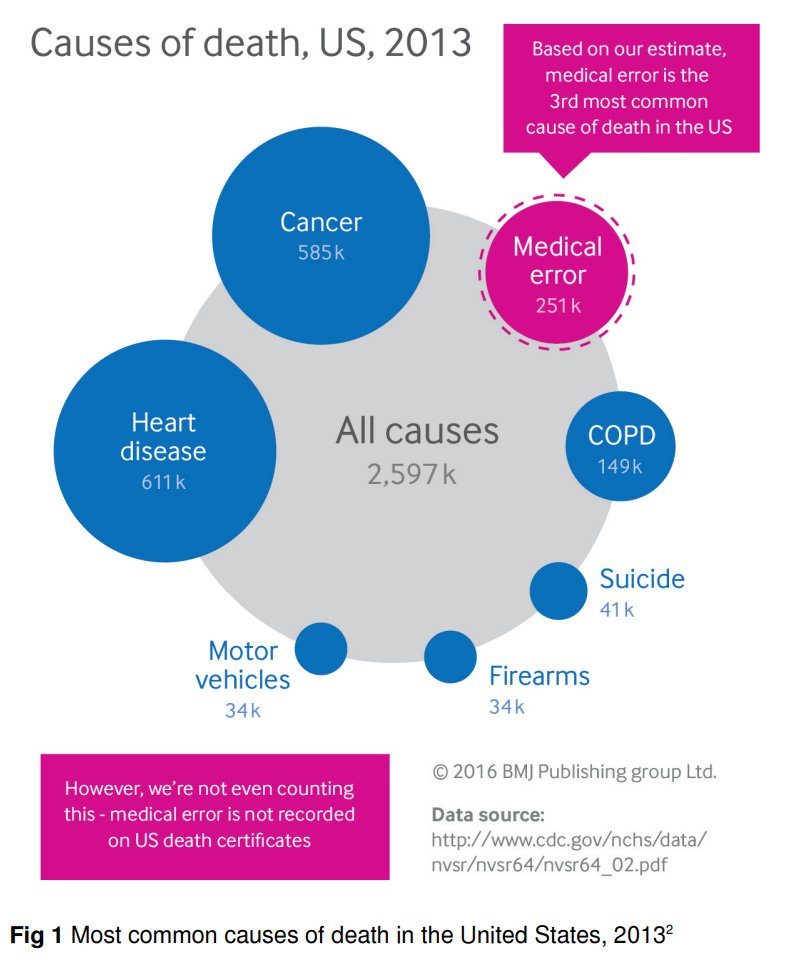
Figure 1: Most common causes of death in the United States, 2013
9. 2022 – HHS Office of Inspector General, “Adverse Events in Hospitals: A Quarter of Medicare Patients Experienced Harm in October 2018.”[12]
Finding: Twenty-five percent of hospitalized Medicare patients experienced harm during their hospital stays, with 43% of harm events deemed preventable—nearly identical to findings from 2010 despite a decade of patient safety initiatives. Medication-related harm was most common (43%).
Significance: This federal government report provided the first updated national incidence rate since 2010, confirming that patient safety had not meaningfully improved. The finding that “little has changed”[13] across twelve years came despite the IOM’s 1999 call to action and the 2010 HHS report.
Conclusion: the cumulative weight of evidence
Taken together, these studies represent nearly 50 years of consistent, peer-reviewed, government-funded, and federally produced evidence that medical care causes a staggering number of preventable deaths each year. The estimates vary by methodology—from 44,000 (IOM’s lower bound) to over 400,000 (James)—but the conclusion is robust across all of them: medical harm is a leading cause of death in the United States.
Yet this conclusion remains absent from official CDC mortality rankings. A death certificate is an opinion, not an objective fact. It records the immediate biological event (cardiac arrest, respiratory failure, sepsis) or the underlying disease being treated (cancer, heart disease, diabetes), but it does not capture the medical error, adverse drug reaction, hospital-acquired infection, or unnecessary procedure that precipitated death. The system is structurally blind to iatrogenic harm.
In addition, a death certificate relies on the International Classification of Diseases (ICD) codes to record the cause of death. As Makary explained in a university press release: “The medical coding system was designed to maximize billing for physician services, not to collect national health statistics, as it is currently being used.”[14]
Even more fundamentally, the death certificate does not—and cannot—reflect the complex cascade of nutritional, environmental, and lifestyle factors that led to that moment. The patient who dies from a heart attack may have spent decades with undiagnosed magnesium deficiency, poor diet, chronic stress, and vitamin D insufficiency—none of which appear on the certificate. By presenting simple statistics as definitive causes, the system misleads researchers, policymakers, and the public about where disease and death actually originate.
The CDC’s official cause-of-death rankings are not maliciously deceptive. They are a product of a coding system designed for a different era and a different purpose. But the effect is the same: medical error, nutritional deficiency, and lifestyle factors remain invisible—and therefore underfunded, understudied, and unaddressed.
The patient who dies from malnutrition is counted as a dementia death. The patient whose vitamin D deficiency contributed to a fatal fall is counted as an accident. The patient whose magnesium deficiency triggered a fatal arrhythmia is counted as a heart disease death. The patient who dies as a result of a reaction to a medication is counted as another death.
The cumulative message of these studies is not that medicine is worthless or that patients should avoid care. Surgery saves lives. Emergency medicine saves lives. But the same system that saves lives also takes them—often preventably, often invisibly, and with little measurable improvement despite decades of attention.
The first step toward solving a problem is acknowledging its existence. The way we keep mortality statistics is primitive and misleading, and it is not helping us understand the true causes of death or what we can do to make people healthier. As the 2013 James study concluded: “Any of these figures demands assertive action.” The 2022 HHS report makes clear that assertive action has not yet come. The question is not whether the evidence exists—it has existed for five decades. The question is whether patients, families, and the public will demand the transparency, accountability, and systemic reform that this evidence warrants.
Significant study quotes
“We can conjecture the range of 60,000 to 140,000 ADR deaths to be probably extremely conservative since we have no data measuring drug-induced deaths in the ambulatory and extended care populations.”[15]
“The estimated number of deaths owing to DRPs [Drug Related Problems] in this analysis ranged from 79.15 to 198,815 deaths.”[16]
“When extrapolated to the over 33.6 million admissions to U.S. hospitals in 1997, the results of the study in Colorado and Utah imply that at least 44,000 Americans die each year as a result of medical errors. The results of the New York Study suggest the number may be as high as 98,000. Even when using the lower estimate, deaths due to medical errors exceed the number attributable to the 8th-leading cause of death. More people die in a given year as a result of medical errors than from motor vehicle accidents (43,458), breast cancer (42,297), or AIDS (16,516).”[17]
“US estimates of the combined effect of errors and adverse effects that occur because of iatrogenic damage not associated with recognizable error include:
• 12,000 deaths/year from unnecessary surgery
• 7,000 deaths/year from medication errors in hospitals
• 20,000 deaths/year from other errors in hospitals
• 80,000 deaths/year from nosocomial infections in hospitals
• 106,000 deaths/year from nonerror, adverse effects of medications.
These total to 225,000 deaths per year from iatrogenic causes.”[18]
“1.5 percent of Medicare beneficiaries experienced an event that contributed to their deaths, which projects to 15,000 patients in a single month [180,000 per year].”[19]
“2.7 million hospitalized Americans each year have experienced a serious adverse reaction. Of all hospitalized patients, 0.32 percent died due to ADRs, which means that an estimated 128,000 hospitalized patients died annually, matching stroke as the 4th leading cause of death. Deaths and serious reactions outside of hospitals would significantly increase the totals.
An analysis conducted in 2011, based on a year of ADRs reported to the FDA, came to similar conclusions: Americans experienced ‘2.1 million serious injuries, including 128,000 patient deaths.’ Other studies reveal that one in every five NMEs [New Molecular Entities][20] eventually caused enough serious harm in patients to warrant a severe warning or withdrawal from the market. Of priority drugs that were reviewed in slightly more than half the normal time, at least one in three of them caused serious harm.”[21]
“Following the IOM report, there was considerable debate over the accuracy of its estimates regarding patient deaths associated with adverse events in hospitals, but whether the true number is 100,000, 200,000, or 400,000 Americans each year is, in a sense, beside the point—any of these figures demands assertive action from providers, legislators, and future patients. Yet, progress on patient safety remains frustratingly slow; nonetheless, one must hope that the present, evidence-based estimate of over 400,000 deaths per year will finally foster an outcry for overdue changes and increased vigilance in medical care to address the problem of harm to patients who come to a hospital seeking only to be healed.”[22]
[23]“We calculated a mean rate of death from medical error of 251,454 per year using studies published since the 1999 IOM report and extrapolating to the total number of U.S. hospital admissions in 2013, though we believe this actually understates the true incidence because the studies rely on errors extractable from documented health records and include only inpatient deaths. While the assumptions made in extrapolating study data to the broader U.S. population may limit the accuracy of our figure, the absence of national data highlights the need for systematic measurement of the problem; comparing our estimate to CDC rankings suggests that medical error is the third most common cause of death in the United States.”[23]
References
1. Patient Safety Action Network, https://www.patientsafetyaction.org/community/john-t-james-ph-d
2. “Could Medical Errors Be No. 3 Cause of Death?” May 4, 2016, https://www.nbcnews.com/health/health-care/could-medical-errors-be-no-3-cause-death-america-n568031
3. Dr. Barry Gustin, “Medication Errors: #3 Cause of Death in U.S.” Dr. Barry Gustin, November 9, 2025, https://barrygustinmd.com/medication-errors-3-cause-of-death-in-u-s
4. Robert B. Talley, MD, and Marc F. Laventurier, “Drug-Induced Illness,” Journal of the American Medical Association, August 19, 1974, vol. 229, no. 8, p. 1043, https://jamanetwork.com/journals/jama/article-abstract/356271
5. Jefferey A Johnson and Lyle Bootman, “Drug-Related Morbidity and Mortality,” Journal of Managed Care Pharmacy, Jan/Feb 1996, vol. 2, no. 1, pp. 39-47, https://www.jmcp.org/doi/pdf/10.18553/jmcp.1996.2.1.39
6. “To Err Is Human Building a Safer Health System,” Institute of Medicine, 1999, p. 1, https://pubmed.ncbi.nlm.nih.gov/25077248
7. Barbara Starfield, MD, MPH, “Is US Health Really the Best in the World?” Journal of the American Medical Association, July 26, 2000, vol. 284, no. 4, pp. 483-485, https://pubmed.ncbi.nlm.nih.gov/10904513
8. Adverse Events in Hospitals: National Incidence Among Medicare Beneficiaries, Department of Health and Human Services, November 2010, pp. 18-19, https://oig.hhs.gov/oei/reports/oei-06-09-00090.pdf
9. Donald W. Light, et al., “Institutional Corruption of Pharmaceuticals and the Myth of Safe and Effective Drugs,” The Journal of Law Medicine & Ethics, September 2013, pp. 590-600, https://www.willhall.net/files/PharmaCorruptionInstitutionalDavidLight.pdf
10. James, John T., PhD, “A New, Evidence-based Estimate of Patient Harms Associated with Hospital Care,” Journal of Patient Safety, September 2013, pp. 122-128, https://journals.lww.com/journalpatientsafety/fulltext/2013/09000/a_new,_evidence_based_estimate_of_patient_harms.2.aspx
11. Professor Martin A Makary, “Medical error-the third leading cause of death in the US,” British Medical Journal, May 2016, https://pubmed.ncbi.nlm.nih.gov/27143499
12. “Adverse Events in Hospitals: A Quarter of Medicare Patients Experienced Harm in October 2018,” May 2022, https://oig.hhs.gov/documents/evaluation/2997/OEI-06-18-00400-Complete%20Report.pdf
13. Persistent Inpatient Harm: the Unremitting Challenge of Patient Safety, Journal of General Internal Medicine, November 2022, https://link.springer.com/article/10.1007/s11606-022-07943-1
14. Dr. Barry Gustin, “Medication Errors: #3 Cause of Death in U.S.” Dr. Barry Gustin, November 9, 2025, https://barrygustinmd.com/medication-errors-3-cause-of-death-in-u-s
15. Robert B. Talley, MD, and Marc F. Laventurier, “Drug-Induced Illness,” Journal of the American Medical Association, August 19, 1974, vol. 229, no. 8, p. 1043, https://jamanetwork.com/journals/jama/article-abstract/356271
16. Jefferey A Johnson and Lyle Bootman, “Drug-Related Morbidity and Mortality,” Journal of Managed Care Pharmacy, Jan/Feb 1996, vol. 2, no. 1, pp. 39-47, https://www.jmcp.org/doi/pdf/10.18553/jmcp.1996.2.1.39
17. “To Err Is Human Building a Safer Health System,” Institute of Medicine, 1999, p. 1, https://pubmed.ncbi.nlm.nih.gov/25077248
18. Barbara Starfield, MD, MPH, “Is US Health Really the Best in the World?” Journal of the American Medical Association, July 26, 2000, vol. 284, no. 4, pp. 483-485, https://pubmed.ncbi.nlm.nih.gov/10904513
19. Adverse Events in Hospitals: National Incidence Among Medicare Beneficiaries, Department of Health and Human Services, November 2010, pp. 18-19, https://oig.hhs.gov/oei/reports/oei-06-09-00090.pdf
20. NMEs are novel, active pharmaceutical ingredients that have not been previously approved for marketing in the United States (or other regulatory markets).
21. Donald W. Light, et al., “Institutional Corruption of Pharmaceuticals and the Myth of Safe and Effective Drugs,” The Journal of Law Medicine & Ethics, September 2013, pp. 590-600, https://www.willhall.net/files/PharmaCorruptionInstitutionalDavidLight.pdf
22. James, John T., PhD, “A New, Evidence-based Estimate of Patient Harms Associated with Hospital Care,” Journal of Patient Safety, September 2013, pp. 122-128, https://journals.lww.com/journalpatientsafety/fulltext/2013/09000/a_new,_evidence_based_estimate_of_patient_harms.2.aspx
23. Professor Martin A Makary, “Medical error-the third leading cause of death in the US,” British Medical Journal, May 2016, https://pubmed.ncbi.nlm.nih.gov/27143499
Image source: RDNE Stock project
Note: The views expressed here do not exclusively represent the views of Materia+ and governing entities.
Check out these recently published articles on Materia+.
Stress is something we all feel. And while it’s a universal feeling...
You’ve likely heard me say this before, protein is foundational. It supports...
From pharmacy shelves to garden rootsBefore the age of flashy drug ads...
Of all the beliefs that quietly shape our lives, this one is...